Originally Posted by Bwana:
Once again, don't come in this thread with some kind of political agenda, or you will be shown the door. If you want to go that route, there is a thread about this in DC.
Originally Posted by Dartgod:
People, there is a lot of good information in this thread, let's try to keep the petty bickering to a minimum.
We all have varying opinions about the impact of this, the numbers, etc. We will all never agree with each other. But we can all keep it civil.
Thanks!
Click here for the original OP:
Spoiler!
Apparently the CoronaVirus can survive on a inanimate objects, such as door knobs, for 9 days.
California coronavirus case could be first spread within U.S. community, CDC says
By SOUMYA KARLAMANGLA, JACLYN COSGROVE
FEB. 26, 2020 8:04 PM
The Centers for Disease Control and Prevention is investigating what could be the first case of novel coronavirus in the United States involving a patient in California who neither recently traveled out of the country nor was in contact with someone who did.
“At this time, the patient’s exposure is unknown. It’s possible this could be an instance of community spread of COVID-19, which would be the first time this has happened in the United States,” the CDC said in a statement. “Community spread means spread of an illness for which the source of infection is unknown. It’s also possible, however, that the patient may have been exposed to a returned traveler who was infected.”
The individual is a resident of Solano County and is receiving medical care in Sacramento County, according to the state Department of Public Health.
The CDC said the “case was detected through the U.S. public health system — picked up by astute clinicians.”
Officials at UC Davis Medical Center expanded on what the federal agency might have meant by that in an email sent Wednesday, as reported by the Davis Enterprise newspaper.
The patient arrived at UC Davis Medical Center from another hospital Feb. 19 and “had already been intubated, was on a ventilator, and given droplet protection orders because of an undiagnosed and suspected viral condition,” according to an email sent by UC Davis officials that was obtained by the Davis Enterprise.
The staff at UC Davis requested COVID-19 testing by the CDC, but because the patient didn’t fit the CDC’s existing criteria for the virus, a test wasn’t immediately administered, according to the email. The CDC then ordered the test Sunday, and results were announced Wednesday. Hospital administrators reportedly said in the email that despite these issues, there has been minimal exposure at the hospital because of safety protocols they have in place.
A UC Davis Health spokesperson declined Wednesday evening to share the email with The Times.
Since Feb. 2, more than 8,400 returning travelers from China have entered California, according to the state health department. They have been advised to self-quarantine for 14 days and limit interactions with others as much as possible, officials said.
“This is a new virus, and while we are still learning about it, there is a lot we already know,” Dr. Sonia Angell, director of the California Department of Public Health, said in a statement. “We have been anticipating the potential for such a case in the U.S., and given our close familial, social and business relationships with China, it is not unexpected that the first case in the U.S. would be in California.”
It is not clear how the person became infected, but public health workers could not identify any contacts with people who had traveled to China or other areas where the virus is widespread. That raises concern that the virus is spreading in the United States, creating a challenge for public health officials, experts say.
“It’s the first signal that we could be having silent transmission in the community,” said Lawrence Gostin, director of the World Health Organization Collaborating Center on National and Global Health Law. “It probably means there are many more cases out there, and it probably means this individual has infected others, and now it’s a race to try to find out who that person has infected.”
On Tuesday, the CDC offered its most serious warning to date that the United States should expect and prepare for the coronavirus to become a more widespread health issue.
“Ultimately, we expect we will see coronavirus spread in this country,” said Nancy Messonnier, director of the CDC’s National Center for Immunization and Respiratory Diseases. “It’s not so much a question of if, but a question of when.”
According to the CDC’s latest count Wednesday morning, 59 U.S. residents have tested positive for the new strain of coronavirus — 42 of whom are repatriated citizens from a Diamond Princess cruise. That number has grown by two since Messonnier’s last count Tuesday, although the CDC was not immediately available to offer details on the additional cases.
More than 82,000 cases of coronavirus have been reported globally, and more than 2,700 people have died, with the majority in mainland China, the epicenter of the outbreak.
But public health leaders have repeatedly reminded residents that the health risk from the novel coronavirus to the general public remains low.
“While COVID-19 has a high transmission rate, it has a low mortality rate,” the state Department of Public Health said in a statement Wednesday. “From the international data we have, of those who have tested positive for COVID-19, approximately 80% do not exhibit symptoms that would require hospitalization. There have been no confirmed deaths related to COVID-19 in the United States to date.”
CDC officials have also warned that although the virus is likely to spread in U.S. communities, the flu still poses a greater risk.
Gostin said the news of potential silent transmission does not eliminate the possibility of containing the virus in the U.S. and preventing an outbreak.
“There are few enough cases that we should at least try,” he said. “Most of us are not optimistic that that will be successful, but we’re still in the position to try.”
It's a ridiculous stretch to say that excess deaths are ever going to be quantified as suspected covid on some kind of aggregate basis. Nor does the NY Times have any authority to decide what is and isn't an official death - so that makes no sense to me either.
What he's handwaving away is that there are some 50k excess deaths over and above the deaths from covid - compared to an average year. That's the real story - especially for the people who assert deaths are being over-counted. He seems to be implying that there's something called "lockdown deaths" (suicides, avoiding surgery?) - which account for the excess deaths. That's a pretty ludicrous claim in its face. You'd better have some strong evidence to support it imo. [Reply]
If anyone's interested in how deaths are actually categorized, and what goes into the official death statistics, this is from a data modeler who works in the medical industry:
Originally Posted by :
Update from Steven Millman, the DC data modeler:
Aug 8th COVID Update: The Three Bears Mortality Update, Is the Death Count Too High, Too Low, or Just Right?
Short version: COVID total US and global death counts are almost certainly undercounts of true mortality. A more clear understanding of how deaths are recorded and counted is essential to understanding the claims being made about over or under-counting.
So tl:dr, but if you want a quick cut-and-paste resource for explaining to people why they're wrong about their particular COVID-19 death count grievance, I'm hoping this will be a good resource for you. Here we go.
There is so much poor information and outright disinformation, I thought it made sense to do an update related to how COVID deaths are collected, counted, reviewed, and published. The most common claims I�m seeing on social media are:
COVID death counts are greatly exaggerated because any death of a COVID positive person is being counted as a COVID death including such unrelated deaths as car accidents, homicides, etc.
COVID death counts are greatly exaggerated because hospitals are financially incentivized to improperly mis-classify deaths as COVID.
COVID death counts are greatly exaggerated because probable COVID deaths are being reported along with confirmed COVID deaths.
COVID death counts (and cases) are being undercounted due to the new reporting system moving data from CDC to HHS.
COVID death counts are being greatly undercounted because death certificates are missing people due to either inadequate testing and/or inaccurate attribution to another cause of death
COVID death counts are on the decline based on the CDC website data but rising in the Hopkins/Worldometer data, so one (or both) of those data sources must be lying.
These six claims are all being used and misused to justify stories folks want to tell. This update will take you through how deaths are actually counted, why they are counted that way, and lay out the facts and falsehoods associated with each of the claims above.
HOW DEATHS ARE COUNTED
The most important thing to understand is that there are two related, but separate ways deaths from disease outbreaks are counted. One is a daily reporting system for tracking epidemics in real time and the other is a longer term process of validating the total deaths over an annualized period (like for the flu) or for the course of a disease outbreak.
Daily monitoring of mortality data allows for both public and governmental entities to get hold of vital information to understanding spread of a disease outbreak and the most important way that this is done is through the surveillance of death certificates which are registered for every death occurring in the United States. All of the mortality data presented in the news, by Johns Hopkins, Worldometer, local and federal government are taken from death certificates. For decades, flu seasons have been tracked this way to get real time information on the severity and geographic distribution of outbreaks. See (https://www.cdc.gov/flu/weekly/index.htm) for more information on how flu mortality is tracked.
Post-outbreak, there is a longer period of evaluation leading to final estimated death counts. This process involves a number of steps, but most important are the validation of the death certificate data and excess mortality modeling. The CDC reviews the incoming data for accuracy throughout the course of the disease and makes adjustments and updates as necessary. Because of this, CDC refers to their death counts as �provisional� until they are published. CDC provisional death counts are always several weeks out of date as a result. After the course of the disease is complete, a secondary process begins in which a total death toll is estimated. That process includes what�s known as excess mortality modeling. Because many deaths from disease outbreaks such as flu and COVID-19 may not be identified as such due to inadequate testing, people dying at home or dying from co-morbid conditions worsened by the disease, statistical methods are used which compare actual deaths to expected deaths during the same period from other relatively stable conditions such as stroke, heart attack, accidents, etc. This final estimate, generally published about two years later, becomes the official death count. With the flu, for example, confirmed cases of flu deaths tend to be four to six times smaller than the ultimately published number.
States and local authorities do NOT determine how to complete death certificates, That guidance comes directly from Health & Human Services and the CDC and they have issued specific rules for how to memorialize COVID-19 deaths. You can find them here: (https://www.cdc.gov/nchs/covid19/cod...-reporting.htm)
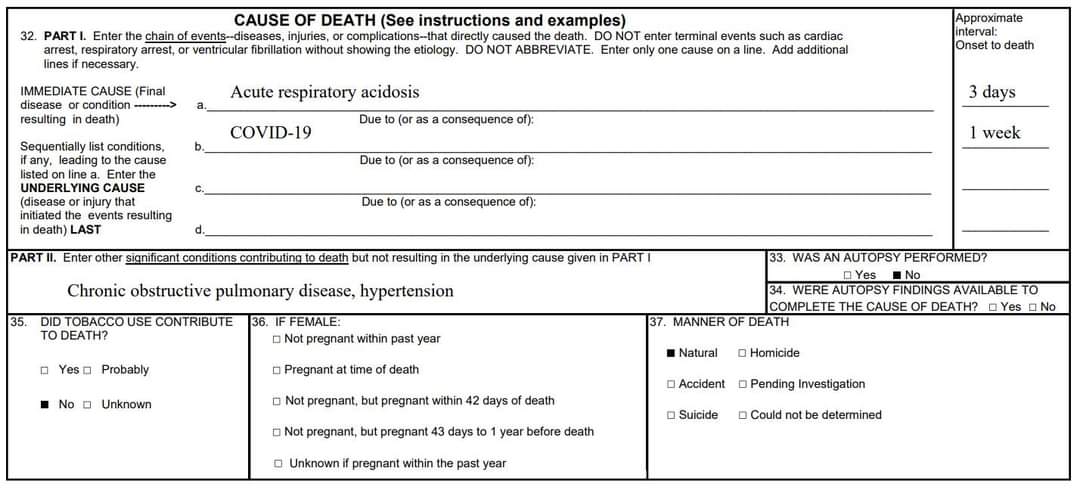
Death certificates have two sections for conditions that could have led to the death of the individual. Part I of the death certificate is for conditions that were a part of the chain of events that led to the death. COVID-19 can be the ultimate cause of death or a step on the way to death. For example, COVID-19 might lead to Acute Respiratory Distress Syndrome which leads to death. In this case, COVID-19 is the underlying cause of death and ARDS is the immediate cause of death. All of those are in Part I. Part II of the death certificate is for other significant conditions which may or may not have contributed to death. In the example above, if the patient had multiple sclerosis for the last ten years that would be included in Part II. Part II conditions would not be generally be reported as causes of death in surveillance.
In order to better track real-time spread of COVID-19, two additional guidelines have been requested by the CDC. (1) Whenever there is a COVID-19 confirmed infection that must be included on the death certificate. If it is a contributory factor in the death it is in Part I of the death certificate. If it is not a contributory factor in the death, it listed in Part II of the death certificate. Only Part I conditions are considered for reporting of death counts. As with the case above, COVID-19 leading to ARDS leading to death is a Part I death included in the COVID-19 death count. A victim of homicide who turns out to be COVID-19 positive would have homicide in Part I and COVID-19 in part II and would NOT be a part of the COVID death count. (2) The second guideline is that here there is a strong probability that COVID-19 was a contributory factor to the death of the individual, but no test was taken it should be included in Part I of the death certificate as �Probable COVID-19.� In order to be listed as probable, the CDC guidelines require a situation in which �the circumstances are compelling within a reasonable degree of certainty.� Here are the specific guidelines from (https://www.cdc.gov/coronavirus/2019...-deaths.html):
1. Meeting clinical criteria AND epidemiologic evidence with no confirmatory laboratory testing performed for COVID-19
2. Meeting presumptive laboratory evidence AND either clinical criteria OR epidemiologic evidence
3. Meeting vital records criteria with no confirmatory laboratory testing performed for COVID19
An example of a probable COVID death provided by the CDC includes a person who died with high fever, acute dry cough and respiratory distress who had been in direct prolonged contact with a known positive COVID patient. These kinds of situations were more prevalent early on when tests were not widely available and were being reserved for live patients with symptoms. Probable cases are evaluated in the CDC provisional data, but may or may not be reported by states in the daily data despite CDC guidance that they do so. About half of the states report probable cases in their daily reporting. (https://www.washingtonpost.com/inves...8e1_story.html)
With that background, let�s move on to the six claims listed above.
1. COVID death counts are greatly exaggerated because any death of a COVID positive person is being counted as a COVID death including such unrelated deaths as those from car accidents, homicides, etc.
UNTRUE. While specific guidance from the CDC requires that COVID-19 appears on the death certificate (causing the confusion), it is only considered in the COVID death count if COVID-19 is in Part I as a contributing cause of the death. A homicide, suicide, car accident, or other clearly unrelated cause of death in a person also positive for COVID-19 would NOT be included in the daily death reporting, or in the eventual published count a year or more after the end of the disease spread. Contributing to this false narrative is a true story that Washington state had been erroneously counting as coronavirus deaths anyone who had tested positive, regardless of cause. Authorities caught the error and corrected it on June 17th decreasing their death count by seven including three homicides, two suicides and two overdoses. That�s just seven out of over 1,200 total deaths in WA state at the time. There is no evidence of widespread misreporting of this nature, there are no states with policies that violate the CDC reporting guidelines, and there is virtually no chance that clerical errors could have a substantial impact on total death counts.
2. COVID death counts are greatly exaggerated because hospitals are financially incentivized to improperly mis-classify deaths as COVID.
UNTRUE. This started with an April 8th comment made by MN State Sen. Scott Jensen, (who is a physician) while being interviewed on Fox News by Laura Ingraham. He raised the idea that the number of COVID-19 deaths may be inflated, saying �Right now Medicare has determined that if you have a COVID-19 admission to the hospital, you�ll get paid $13,000. If that COVID-19 patient goes on a ventilator, you get $39,000, three times as much. Nobody can tell me after 35 years in the world of medicine that sometimes those kinds of things impact on what we do.� In a later interview, however, Jensen said he did not think that hospitals were intentionally misclassifying cases for financial reasons. Either way, none of the allegations made relate to the cause of death on the death certificate, only the diagnosis code listed as the reason for treatment. Further, doctors and medical examiners are responsible for filling out death certificates, not hospitals. Finally, it should be noted that the normal reimbursements under Medicare for respiratory infections and inflammations with major comorbidities or complications in 2017 was $13,297 and for more severe hospitalizations, typical Medicare payment with ventilator support was $40,218. The current payments to hospitals for COVID patients are essentially similar to typical rates.
3. COVID death counts are greatly exaggerated because probable COVID deaths are being reported along with confirmed COVID deaths.
UNTRUE: Only about half of the states even include probable deaths in their reporting despite CDC requests that they do so. Further, the proportion of probable deaths among all COVID deaths is very small. There is an excellent description here: (https://www.nytimes.com/interactive/...eath-toll.html)
4. COVID death counts (and cases) are being undercounted by the Administration through the change to the new reporting system moving data from CDC to HHS.
UNTRUE: The reporting system that changed from the CDC to HHS does not actually include either case or mortality data, so could not be responsible for changes in COVID death counts. That system only includes hospital data such as available beds, ICU beds, available medical staff, etc. For my details, see my earlier Fact Check on this subject at: https://www.facebook.com/steven.mill...57207024331821
5. COVID death counts are being greatly undercounted because death certificates are missing people due to either inadequate testing and/or inaccurate attribution to another cause of death
PROBABLE: There is nothing unusual about death certificates from disease epidemics being undercounts of the true death rate as described above, which is one of the reasons it takes so long to publish official death counts from annual flu. There are many potential reasons for under-reporting including people who died from related conditions (such as heart or respiratory disease), missed diagnoses due to lack of testing (especially early in the pandemic). The Journal of the American Medical Association website (JAMANetwork) published research in July which estimated as much as a 35% undercount in cases at the time. (https://jamanetwork.com/journals/jam...rticle/2768086). This is much lower than the typical undercount in deaths associated with flu, likely because of the greatly enhanced scrutiny of the novel COVID-19 pandemic. Another excellent treatment of why we are likely undercounting the number of deaths from COVID-19 and how many can be found on the CDC�s website at (https://www.cdc.gov/nchs/nvss/vsrr/c...ess_deaths.htm).
6. COVID death counts are on the decline based on the CDC website data but rising in the Hopkins/Worldometer data, so one (or both) of those data sources must be lying.
UNTRUE: As described above, the CDC posts PROVISIONAL counts for COVID-19, pending review and validation. The deaths reported here are, by their nature, filled in over a much longer period of time than the daily reporting system. Because it can take weeks for the data to fill in completely, the CDC provisional data for the most recent time periods always presents lower than the weeks preceding. This is abundantly clear if you look at the CDC website were these data are posted. The CDC website makes the following statements about the provisional counts: (1) �Provisional counts are not final and are subject to change. Counts from previous weeks are continually revised as more records are received and processed.� (2) �Provisional data are not yet complete. Counts will not include all deaths that occurred during a given time period, especially for more recent periods. However, we can estimate how complete our numbers are by looking at the average number of deaths reported in previous years.� (3) �Death counts should not be compared across states. Some states report deaths on a daily basis, while other states report deaths weekly or monthly.� https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
Originally Posted by AustinChief:
Without doing any actual research on it, I would guess he is referring to people(media) referring to all excess deaths that are related to the lockdowns as covid deaths. For example, if there are excess suicides or domestic violence deaths or even deaths such as heart attacks that could have been prevented that can be attributed to the lockdowns... those would be classified as "Covid related deaths." It certainly seems that is the direction the NYT is heading but again I am not terribly interested in diving into this since I have already written off most of the media regarding this entire topic.
Originally Posted by TLO:
Yes. The only other thing I'll add is that states are also going back and reporting deaths that occurred in some instances many months ago which end up going on a daily total for today/tomorrow/etc.
I give up with a lot of the reporting. I watch the Worldometers and what I saw thankfully, was cases spike to almost double than what they were during NY and deaths had 1 day of scratching 1,500 and again it was largely and almost all elderly just as it was before.
That does not downplay nor take away from those lives but the media and some others I won't name have gone on a rant the last few weeks about how we were going to see NY all over again and worse. The media is going crazy now not only over cases but suddenly kids and school and all that. We know what is behind a lot of that and we can't get into that here.
Suffice it to say we saw an expected rise in cases with re-opening and we saw a few states get tagged, like AZ, CA, TX and FL and with all that we never saw NY type results, thankfully. I don't know that there is a need to start freaking out every time a kid tests positive and close schools and what not.
I have said all along and will stand by it still, when the hospitals get ran on then the local area needs to shut down. Until then life has to go on as much as we can though with precautions.
I await the criticism from the standard chorus line of how I don't care, I hate old people, bla, bla ,bla. [Reply]
And relating to schools at least here locally and in the state of Kansas, when the first child dies this year from influenza it will be 1 more than has died from Covid. [Reply]
Originally Posted by petegz28:
And relating to schools at least here locally and in the state of Kansas, when the first child dies this year from influenza it will be 1 more than has died from Covid.
Source?? :-) you mean you don't know? I will correct myself slightly as yesterday they listed an 18 year old. No wonder I keep your pedantic ass on iggy. Take you off for 2 secs and there you are with your same dumb shit. The article you referenced doesn't state any age and you thought you had something because of the word pediatric. It was a 20 year old that died that weekend.
Originally Posted by petegz28:
Source?? :-) you mean you don't know? I will correct myself slightly as yesterday they listed an 18 year old. No wonder I keep your pedantic ass on iggy. Take you off for 2 secs and there you are with your same dumb shit. The article you referenced doesn't state any age and you thought you had something because of the word pediatric. It was a 20 year old that died that weekend.
Originally Posted by Donger:
There you go. I'm well-aware that pediatric covers up to 18.
Except the article you linked was for a 20 year old you dumb ass. The 18 year old passed away this weekend. You aren't well aware of a fucking thing. [Reply]
Originally Posted by petegz28:
Except the article you linked was for a 20 year old you dumb ass. The 18 year old passed away this weekend. You aren't well aware of a ****ing thing.
I doubt that a doctor would classify a 20 year old as a pediatric patient.
Anyway, I think everyone knows that COVID-19 isn't very lethal to young people. So, what's your point? [Reply]
Originally Posted by Donger:
I doubt that a doctor would classify a 20 year old as a pediatric patient.
Anyway, I think everyone knows that COVID-19 isn't very lethal to young people. So, what's your point?
I don't give a fuck what you doubt. Until Friday the youngest person in KS to die was 20. And it was the weekend of your article. It was the talk among all of the local hospitals.
Originally Posted by petegz28:
I don't give a **** what you doubt. Until Friday the youngest person in KS to die was 20. And it was the weekend of your article. It was the talk among all of the local hospitals.
Considering the amount of fail that you've demonstrated in this thread, I'll be happy to tacitly give you one win if it makes you feel better about your worth. [Reply]
{kind=link}
{kind=link}
{kind=link}