Originally Posted by Bwana:
Once again, don't come in this thread with some kind of political agenda, or you will be shown the door. If you want to go that route, there is a thread about this in DC.
Originally Posted by Dartgod:
People, there is a lot of good information in this thread, let's try to keep the petty bickering to a minimum.
We all have varying opinions about the impact of this, the numbers, etc. We will all never agree with each other. But we can all keep it civil.
Thanks!
Click here for the original OP:
Spoiler!
Apparently the CoronaVirus can survive on a inanimate objects, such as door knobs, for 9 days.
California coronavirus case could be first spread within U.S. community, CDC says
By SOUMYA KARLAMANGLA, JACLYN COSGROVE
FEB. 26, 2020 8:04 PM
The Centers for Disease Control and Prevention is investigating what could be the first case of novel coronavirus in the United States involving a patient in California who neither recently traveled out of the country nor was in contact with someone who did.
“At this time, the patient’s exposure is unknown. It’s possible this could be an instance of community spread of COVID-19, which would be the first time this has happened in the United States,” the CDC said in a statement. “Community spread means spread of an illness for which the source of infection is unknown. It’s also possible, however, that the patient may have been exposed to a returned traveler who was infected.”
The individual is a resident of Solano County and is receiving medical care in Sacramento County, according to the state Department of Public Health.
The CDC said the “case was detected through the U.S. public health system — picked up by astute clinicians.”
Officials at UC Davis Medical Center expanded on what the federal agency might have meant by that in an email sent Wednesday, as reported by the Davis Enterprise newspaper.
The patient arrived at UC Davis Medical Center from another hospital Feb. 19 and “had already been intubated, was on a ventilator, and given droplet protection orders because of an undiagnosed and suspected viral condition,” according to an email sent by UC Davis officials that was obtained by the Davis Enterprise.
The staff at UC Davis requested COVID-19 testing by the CDC, but because the patient didn’t fit the CDC’s existing criteria for the virus, a test wasn’t immediately administered, according to the email. The CDC then ordered the test Sunday, and results were announced Wednesday. Hospital administrators reportedly said in the email that despite these issues, there has been minimal exposure at the hospital because of safety protocols they have in place.
A UC Davis Health spokesperson declined Wednesday evening to share the email with The Times.
Since Feb. 2, more than 8,400 returning travelers from China have entered California, according to the state health department. They have been advised to self-quarantine for 14 days and limit interactions with others as much as possible, officials said.
“This is a new virus, and while we are still learning about it, there is a lot we already know,” Dr. Sonia Angell, director of the California Department of Public Health, said in a statement. “We have been anticipating the potential for such a case in the U.S., and given our close familial, social and business relationships with China, it is not unexpected that the first case in the U.S. would be in California.”
It is not clear how the person became infected, but public health workers could not identify any contacts with people who had traveled to China or other areas where the virus is widespread. That raises concern that the virus is spreading in the United States, creating a challenge for public health officials, experts say.
“It’s the first signal that we could be having silent transmission in the community,” said Lawrence Gostin, director of the World Health Organization Collaborating Center on National and Global Health Law. “It probably means there are many more cases out there, and it probably means this individual has infected others, and now it’s a race to try to find out who that person has infected.”
On Tuesday, the CDC offered its most serious warning to date that the United States should expect and prepare for the coronavirus to become a more widespread health issue.
“Ultimately, we expect we will see coronavirus spread in this country,” said Nancy Messonnier, director of the CDC’s National Center for Immunization and Respiratory Diseases. “It’s not so much a question of if, but a question of when.”
According to the CDC’s latest count Wednesday morning, 59 U.S. residents have tested positive for the new strain of coronavirus — 42 of whom are repatriated citizens from a Diamond Princess cruise. That number has grown by two since Messonnier’s last count Tuesday, although the CDC was not immediately available to offer details on the additional cases.
More than 82,000 cases of coronavirus have been reported globally, and more than 2,700 people have died, with the majority in mainland China, the epicenter of the outbreak.
But public health leaders have repeatedly reminded residents that the health risk from the novel coronavirus to the general public remains low.
“While COVID-19 has a high transmission rate, it has a low mortality rate,” the state Department of Public Health said in a statement Wednesday. “From the international data we have, of those who have tested positive for COVID-19, approximately 80% do not exhibit symptoms that would require hospitalization. There have been no confirmed deaths related to COVID-19 in the United States to date.”
CDC officials have also warned that although the virus is likely to spread in U.S. communities, the flu still poses a greater risk.
Gostin said the news of potential silent transmission does not eliminate the possibility of containing the virus in the U.S. and preventing an outbreak.
“There are few enough cases that we should at least try,” he said. “Most of us are not optimistic that that will be successful, but we’re still in the position to try.”
Originally Posted by dirk digler:
Yep it seems to be random on who it affects which makes me think there is some immunity, genetics, blood types that offer some protection.
The only other thing I could think of is she wasn't wearing much PPE back in March and maybe got it early and the antibodies are now gone so the tests can't detect it. I don't know much about these antibody tests to say either way though.
Antibody tests are super unreliable. Especially with false negatives. Also people with no or mild symptoms often don't develop detectable antibodies. [Reply]
Originally Posted by Ebolapox:
I'm a geneticist. I tell students on one of the first relevant lessons that we have 20-25000 different genes. I don't even get to isoforms (same protein, different structure b/c of exon splicing differences). there are over 250 different genes that cause old-age blindness (retinitis pignemtosa: overly simplified, most are old age... some young age). over 1500 that control neurological function (likely more than that with snRNAs and other small RNA species that we barely or don't understand now--all are likely dealing with protein control of some sort, or maybe epigentic stuff that's nuts).
we're incredibly complex and have hundreds of thousands of moving parts (I didn't even get to how our environment comes into play, except kinds: epigenetics). it's not a shocker that something unprecedented like this has many facets and is the ultimate moving target.
The human body can be extremely resilient and fragile all at the same time. [Reply]
Originally Posted by :
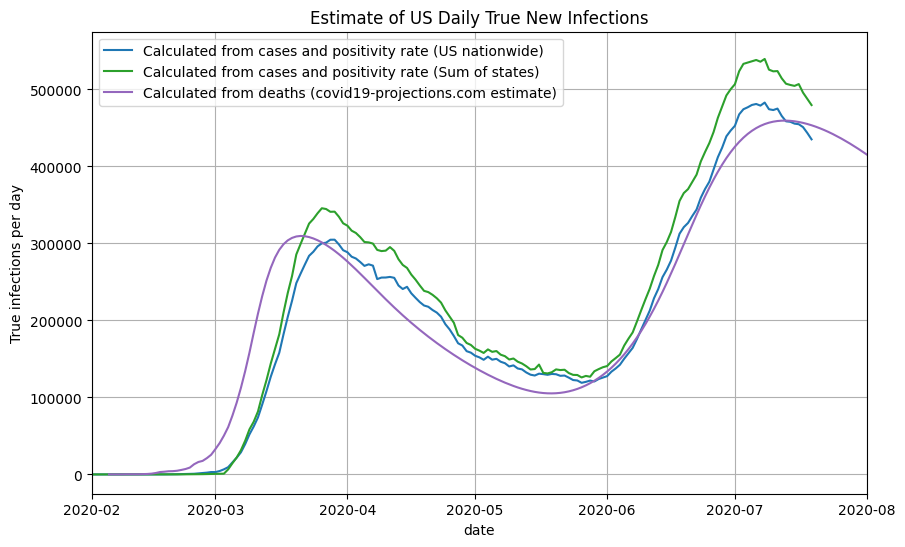
Knowing the true number of people who are infected with COVID-19 in the US is an essential step towards understanding the disease. But estimating this number is not a simple task. The true number of infections is many times greater than the reported number of cases in the US because the majority of infected individuals do not get tested due to several reasons: 1) they are asymptomatic, 2) they are only mildly symptomatic, 3) they do not have easy access to testing, or 4) they simply do not want to.
On this page, we introduce a simple square root function to estimate the true prevalence of COVID-19 in a region based on only the confirmed cases and test positivity rate: true-new-daily-infections = daily-confirmed-cases * (16 * (positivity-rate)^(0.5) + 2.5). We will also introduce the implied infection fatality rate (IIFR), which is a metric derived by taking a region’s reported deaths and dividing it by the true infections estimate (after accounting for lag).
Using this method, we estimate that the true number of new infections peaked at close to 500,000 new infections per day in July, compared to 300,000 new infections per day in March. This means that the peak of infections after reopening is 60% higher than the initial peak in March. In total, by the end of July 2020, we estimate over 35 million (1 in 10) Americans have been infected at some point by the SARS-CoV-2 virus.
Originally Posted by :
Once we have a reasonable estimate of the true number of newly infected individuals per day, we can use the reported deaths to compute the implied infection fatality rate (IFFR). The IIFR for the US was above 1% in March, stabilized at around 0.6% in April-May before decreasing to ~0.25% in July. Note that our IIFR estimate does not take into account excess/unreported COVID-19 deaths, so it is likely a lower bound for the true IFR. This is further explained below.
This meshes with everything else I've been reading. Of course the main driver of IFR decreasing is younger/healthier people getting it while older/at-risk people isolate much better than they were back in Feb/March.
Originally Posted by :
Note that our use of the term infection fatality rate (IFR) refers to true deaths divided by true infections. It is not age-adjusted. As a result, if there is an increasing prevalence of the disease in a younger population, then the IFR will decrease, despite the deadliness of the virus remaining unchanged among a particular age group. It is likely that the fatality rate for a given age group have not changed significantly.
Originally Posted by Ebolapox:
I'm a geneticist. I tell students on one of the first relevant lessons that we have 20-25000 different genes. I don't even get to isoforms (same protein, different structure b/c of exon splicing differences). there are over 250 different genes that cause old-age blindness (retinitis pignemtosa: overly simplified, most are old age... some young age). over 1500 that control neurological function (likely more than that with snRNAs and other small RNA species that we barely or don't understand now--all are likely dealing with protein control of some sort, or maybe epigentic stuff that's nuts).
we're incredibly complex and have hundreds of thousands of moving parts (I didn't even get to how our environment comes into play, except kinds: epigenetics). it's not a shocker that something unprecedented like this has many facets and is the ultimate moving target.
And here I thought it was just that the medical professionals are all dumbasses who either don't know shit, or are lying (/sarcasm) [Reply]
Originally Posted by O.city:
The more we go along with this the more a lot of our moves and things we�re doing are more �illusion of control� vs actually doing any good
Originally Posted by O.city:
The more we go along with this the more a lot of our moves and things we�re doing are more �illusion of control� vs actually doing any good
Want irony? KS said today that the counties that adopted the mask mandate have see a dramatic drop in cases and the counties that did not have not see any drop. The data might suggest otherwise as there was a rise in cases in JoCo though we adopted the mask mandate. In fact cases were going up so mucin the state that last week the Governor threatened to lock us down again. Now everywhere I go I see almost everyone wearing a mask. But everyone I know that lives around me swears no one wears a mask wherever they go. [Reply]
Pottawatomie and Wabaunsee Counties both held their County Fairs with "limited activities" the last week of July. Yesterday the Wab.Co. Health Department issued this:
August 05, 2020
For Immediate Release:
Anyone who attended the Wabaunsee County Fair, July 24th- 27th, and/or fair activities should monitor themselves for COVID symptoms. An individual(s) who attended the fair and accompanying activities, including the rodeo, lawn chair concert, parade, and feed, has tested positive.....
We don't have protests we have county fairs. [Reply]
Originally Posted by KS Smitty:
Pottawatomie and Wabaunsee Counties both held their County Fairs with "limited activities" the last week of July. Yesterday the Wab.Co. Health Department issued this:
August 05, 2020
For Immediate Release:
Anyone who attended the Wabaunsee County Fair, July 24th- 27th, and/or fair activities should monitor themselves for COVID symptoms. An individual(s) who attended the fair and accompanying activities, including the rodeo, lawn chair concert, parade, and feed, has tested positive.....
We don't have protests we have county fairs.
See, that's the problem. If you tear shit down with fire you scare the Rona away. Also we now have evidence that if you attend a funeral for a politician you can assume you are Rona-free.
See, you need to pick and choose your activities accordingly. [Reply]
Originally Posted by loochy:
If you can't even tell that you are sick then you are asymptomatic
I agree. And that means even if you think your allergies are acting up. I don't know where they draw the line of asymptomatic vs. symptoms so mild you chalk it up to something other than being sick but you still have symptoms? [Reply]
Coronavirus: Why everyone was wrong
The immune response to the virus is stronger than everyone thought
The original article was published in the Swiss magazine Weltwoche (World Week) on June 10th. The author, Beda M Stadler is the former director of the Institute for Immunology at the University of Bern, a biologist and professor emeritus.
The fairy tale of no immunity
From the World Health Organisation (WHO) to every Facebook-virologist, everyone claimed this virus was particularly dangerous, because there was no immunity against it, because it was a novel virus. Even Anthony Fauci, the most important advisor to the Trump administration noted at the beginning at every public appearance that the danger of the virus lay in the fact that there was no immunity against it. Tony and I often sat next to each other at immunology seminars at the National Institute of Health in Bethesda in the US, because we worked in related fields back then. So for a while I was pretty uncritical of his statements, since he was a respectable colleague of mine. The penny dropped only when I realised that the first commercially available antibody test [for Sars-CoV-2] was put together from an old antibody test that was meant to detect Sars-1.
For every other disease that doesn’t afflict a certain group of people, we would come to the conclusion that that group is immune. When people are sadly dying in a retirement home, but in the same place other pensioners with the same risk factors are left entirely unharmed, we should also conclude that they were presumably immune.
But this common sense seems to have eluded many, let’s call them “immunity deniers” just for fun. This new breed of deniers had to observe that the majority of people who tested positive for this virus, i.e. the virus was present in their throats, did not get sick. The term “silent carriers” was conjured out of a hat and it was claimed that one could be sick without having symptoms. Wouldn’t that be something!
{kind=link}
{kind=link}